I know a lot of my close family and friends are concerned about my upcoming gastric bypass surgery so I want to put some information out there. I’ve been educated by multiple people including doctors, dietitians, to even one of the four surgeons that will perform the procedure. This surgery is now very low risk, the surgeon joked he could “do it with his eyes closed” and it’s less invasive than gall bladder removal. University of Michigan has one of the best programs for anyone considering weight loss surgery and I can testify that it is the most organized process I’ve ever been involved in. This blog is not going to be about the process to get surgery but about the surgery itself. An update and more thorough blog on the journey to surgery will be coming soon.
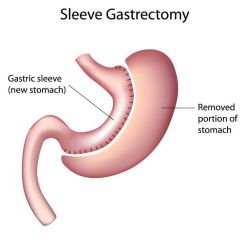
First off, there are two types of weight loss surgery UM does: Roux en Y and the gastric sleeve surgery. Roux en Y is the more intricate surgery where they remove most of your stomach and connect what is left to the middle of your small intestine. The gastric sleeve surgery is where they cut your stomach vertically and remove about 85% of your stomach. There is no rerouting in gastric sleeve surgery and it is performed laparoscopically meaning there will be no large cuts but a few small sized puncture holes.
UM does this really cool thing where they take the results of people that are similar to you (height, weight, ethnicity, age, etc.) and pull data to project your weight loss and complication rate based on that. My complication rate is 4.06% for minor complications, 1.07% for major complications, and .05% for death. I was intrigued to find the differences in complication rates for other people in the first support group meeting. Some people’s were as high as 20% for minor complications.
The surgeon was extremely helpful and knowledgeable. One of his colleagues is currently doing a study to find out WHY gastric surgery works so well. They’ve concluded it’s NOT the caloric restriction solely as they’ve compared people with gastric and without who’ve eaten the same amount of calories with similar activity levels and the gastric patient still loses significantly more (and keeps it off). They believe it has something to do with the portion of the stomach that was removed– like that portion contained all of the hormones or chemical reactions that caused weight gain.
The surgery will take about an hour and a half and I will be inpatient for 2-3 days mostly for pain management and monitoring. The recovery is pretty quick at around 2 weeks although fatigue, nausea and vomiting can last a bit longer. There were a few people in attendance of my support group meeting who had already had the surgery and they said they were able to function normally within the first week. I am a baby when it comes to stomach pain so we shall see. I will have to take a multivitamin, calcium supplements and a vitamin B12 for the rest of my life. (Just an FYI, roux n y requires B12 injections as there’s very little to no digestion of B12 after the rerouting of the stomach) I’ve already started taking my vitamins about 4 months ago so it won’t be a major change for me. I won’t get a surgery date for a while but I will be blogging throughout this entire process.
Until next time.
